
Our Co-Founder and CEO, Roy Bejarano, recently had the opportunity to speak with David Kovel, a respected Scale Healthcare technology and operations leader, about scaling IT and data functions for provider platforms. David has deep expertise in the areas of technology architecture, information systems planning, strategic deployment of information technology, operational and business process improvement, application development and implementation, business sourcing services integration, organization development, and change management.
A seasoned healthcare technology practitioner, David has served as a senior executive for health care organizations. He has acted as the interim CIO and senior technology leader for a variety of provider platforms nationally. As a health care domain expert, David blends an ability to see the big picture while maintaining his passion for the tactical details that ensure programmatic success.
Building the Ideal IT Team for Your Provider Platform
Roy Bejarano: What does the ideal target provider platform IT / Data Management department look like? Define IT as broadly as you would like.
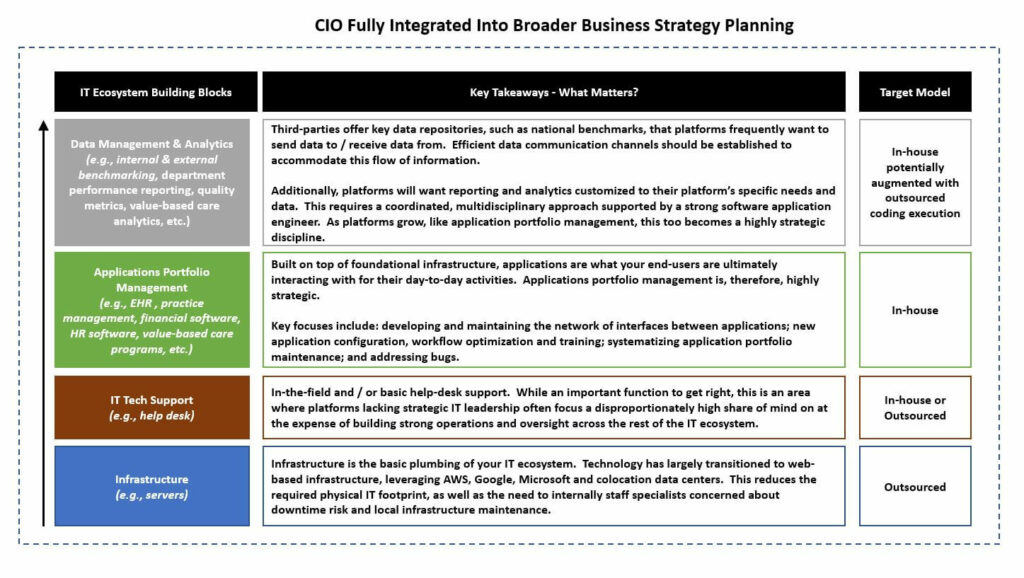
David Kovel: IT departments are not defined simply as technology support any more. They are more broadly missioned and inclusive of a network of internal and outsourced teams and infrastructure. Visually, a fully developed IT department can be described from the ground up.
RB: Based on this extensive list of responsibilities and implied expertise, would it be fair to say that IT / Data is generally underinvested in across physician platforms?
DK: Yes. Definitively. The reality is that very few provider platforms have invested in more than 50% of this list. The majority of platforms are under-resourced and just beginning to appreciate the benefits of Applications Portfolio Management and Data Management & Analytics. Lack of leadership, planning and funding are why systems aren’t being scaled to maximize patient experience, optimize and automate workflows, and leverage data efficiently as source for decision-making.
Common indications that you are underinvested: frequent IT-related inefficiencies; frustrated providers and poor flow of information across the organization; bad IT investments or confused IT investment strategy; no IT budget; no 1- to 5-year IT strategy roadmap. To scale operations and remain competitive, a small IT team focused on tech support or an ad-hoc strategic approach will not produce results that propel the platform forward.
RB: When I think about a lot of the IT departments in platforms we come across, that’s quite an overwhelming investment / build that they have ahead of them.
DK: Well, you don’t start out with the finished product and I wouldn’t recommend solving for every position across every platform. The full ecosystem gets built and matures incrementally over time.
You need to establish a bridge or pathway to the target structure that is responsive to the organization’s financial, political and cultural reality. Yes, “where do I want to be over the near-, mid- and long-term”? But, also, what departmental structure, team size and investments are appropriate for where my platform is today?
Here again, I think the concept is easier to digest visually. Below is an illustrative mapping of what an IT department looks like over time – beginning with supporting a smaller physician group and then expanding the IT team’s functional scope as the platform scales in terms of number of providers, patients, service lines, and geographies covered.

Tracking IT Performance at a Provider Platform
RB: Moving from IT team to IT performance, let’s imagine you are the CIO of a physician platform and are presenting to your Board on IT department performance. What is included in your IT executive summary dashboard? In other words, how does the Board and executive leadership team know if its IT department is doing a good job in supporting and adding value to the enterprise?
DK: Each of the IT sub-departments reporting to the CTO / CIO will enable the system’s leader to address a complex role of addressing current systems performance, delivery of analytics supporting the decision makers in other parts of the organization, and architecting the future state of the platform’s business plan. The CTO / CIO should be collaborating regularly with the CFO and COO, and should ultimately be reporting to the President / CEO, as well as presenting to the Board.
At the Board-level, I would be focused on an executive summary report covering:
- Operational KPIs
- IT staff turnover
- Help desk call volume and service levels for addressing (i.e., resolution time). As a quick cheat when I evaluate a new platform, I look at help desk tickets. How quickly are user needs met? This tells me a lot about the stability of the architecture.
- Number of IT complaints across all departments
- Application and infrastructure maintenance inventory confirming proactive upgrade / maintenance schedule and completion status
- Provider, staff and patient satisfaction with the IT department and systems
- Strategy
- Are the Board and executive teams empowered with user-friendly, data-driven reports? If not, what IT development projects could help the other departments improve their reporting to drive better decision-making discourse. What is the implementation status of each?
- What is the inventory and execution status across all on-going and contemplated strategic IT initiatives – i.e., the active and in-active IT pipeline
- Summary of amounts invested in IT development for active projections
- IT financial budget and budget variance
- Lastly, but perhaps most importantly, an assessment of what new IT investment options we should be considering. It’s the solutions you don’t currently have that will define the future of your organization.
Investing in IT for Your Provider Platform
RB: Often times, we see groups struggle with investing in IT because much of IT investment appears speculative to the novice – it’s a Catch 22. Will the new application actually work? How does a qualified IT team prevent time and financial waste? A few common examples where we have seen waste:
- Failed interfaces between disparate IT systems
- The next shiny prepacked third-party application that sounds nice in theory but yields little adoption and ambiguous effectiveness in reality
- Proprietary application development, where the universe of possibilities is both endless and tantalizing, and the outcomes are inherently uncertain given the development aspect of the initiative
DK: Department interdependence complicates this process, and that is where it’s not good enough to just have a great IT department. A poor IT department will certainly slow your organization down, but a great one on its own can’t speed you up. You need strong performance and collaboration across departments – it’s all co-dependent.
A poor IT department will certainly slow your organization down, but a great one on its own can’t speed you up. You need strong performance and collaboration across departments – it’s all co-dependent.
Accordingly, approach de-risking new IT investments by establishing an IT Investment Committee with representation from IT, clinical, operations, financial and physician communities. The goal is to produce a thoughtful and analytically-driven scorecard of the particular investment. Is the investment solving a critical need? What is our confidence that the application will adequately meet the business need if it is deployed? Have others implemented the solution before or are we beta testing? How much is the anticipated investment? What is the implementation timeline and complexity? Have we clearly defined what success looks like and how we will measure it post-implementation?
Further, IT initiatives succeed or fail based on user-adoption. Therefore, for each investment initiative, I like to see a true initiative champion from each relevant stakeholder community – that is, someone with the desire, influence and accountability to drive ultimate adoption.
From an IT-specific perspective, during the evaluation phase, build out the technical integration plan. Where does the application sit and what communication needs to occur with other applications in order for the project to succeed?
RB: How do you evaluate projects ex-post to determine success, lessons learned, etc.?
DK: Financial success is measured against the value proposition of original business case – however, the full appreciation of ROI and a successful, tangible target outcome is achieved with platform performance improvements plus provider and staff satisfaction plus user-adoption.
This relates back to the Board executive summary dashboard discussed earlier. The job doesn’t end at implementation. Visibility to IT initiatives through true stabilization is required to analyze how the investment, implementation and integration processes played out.
RB: It is a common refrain that there is no perfect EHR / PM system. Given that, what criteria do you use for evaluating these systems from an IT perspective? I often hear in EHR selection that the implementation phase was highly disruptive and the end result not exactly what was promised. How do you avoid that?
DK: Firstly, the system vetting and selection process is usually too narrow – it can’t be led by any one provider, administrator or IT expert. You will need the full range of users involved and get their buy-in. Technology vendors are now frequently incorporating business processing services and other partners to provide a comprehensive offering that impacts the experience of all users.
Additionally, changing systems is not easy and providers require clear communication regarding clinical information conversion, so that expectations are managed. Providers tend to value a lot of patient content/history on the legacy system. But, typically migrating old data is highly cost ineffective, and some will get left behind.
Finally, a provider platform must consider its external constituencies – patient engagement and satisfaction can be closely tied to the utilization of the EMR/PM system. Data exchange capabilities with the payor community will become system requirements for more sophisticated contracting and integration with ancillary clinical providers.
RB: What’s ironic is that with IT being so technical, it often ends up being one of the most remote and introverted departments. And yet, its relevance and its potential value add applies to every other platform division – from payor contracting, to provider performance and clinical operations, to credentialing, to financial reporting and revenue cycle management, to HR/human capital management and to patient interaction.
DK: The list of departments affected and reliant on strong IT is extensive, so IT senior leadership are amongst the most important hires in the organization. And yet for many CEOs, the IT department is often largely overlooked, somewhat misunderstood, and typically underutilized. IT senior leaders should be included in – and sometimes driving – strategic discussion across your enterprise. As an example, IT senior leadership should be part of internal & external payor contracting review. Payors want to see who in the organization is taking responsibility for data gathering and deliver.
IT senior leaders should be included in – and sometimes driving – strategic discussion across your enterprise.
RB: What are the biggest risks? Where do practices commonly go wrong and what is the cost / performance impact of “getting it wrong”?
DK: I’ve seen platforms overinvest – bought in by vendor salesmanship only later realizing it was a luxury purchase, not a necessity, and didn’t really transform the way the business functions and creates value. This is unfortunately what prevents platforms from investing correctly. The only cure is to truly develop IT leadership expertise that is fully integrated into the broader platform strategy and operations. For many, IT remains a black box. Here, I think a group like Scale Physician Group can play a key role in bringing clarity, experience and expertise as group’s contemplate how IT fits in within their platform and how to achieve their goals.
RB: Have you seen examples where IT has really helped standardize performance and improve enterprise-wide communication / clarity as a group scaled?
DK: Yes. The best platforms can point to great feedback and experience from patients, providers, staff, management and payors, and finally the Board who is asking for longer-term strategic IT initiatives.
Regardless of provider platform size or stage of development, IT / data management is a critical function that requires seasoned leadership, strategic roadmap clarity, on-going C-Suite / Board oversight and a prudent level of investment. If IT remains a nebulous function that generally gets share of mind only when problems occur, that may be a sign that your platform has not transitioned beyond tactical IT support to develop a strategic and value enhancing IT / data management program. Scale brings C-Suite IT experience to help your platform assess and develop its IT / data strategy, clearly define a strategic IT roadmap, integrate IT across your broader organization, and develop a team that is suitable for your platform’s size and stage of development.
We would like to thank David for his time and for sharing his expertise with us.